Postsurgical intra ocular pressure control comparing Deep sclerectomy Vs Trabeculectomy both with MMC in Tripoli eye Hospital 2021-2022
التحكم في ضغط العين بعد الجراحة: مقارنة بين استئصال الصلبة العميق واستئصال التربيق، وكلاهما باستخدام الميتومايسين C في مستشفى طرابلس للعيون، 2021–2022
Eman S M Amr1, Algharib Alshraa1, DR Mansour Jeneva1
1 Tripoli Eye Hospital, Libya.
DOI: https://doi.org/10.53796/hnsj76/1
Arabic Scientific Research Identifier: https://arsri.org/10000/76/1
Volume (7) Issue (6). Pages: 1 - 8
Received at: 2026-05-10 | Accepted at: 2026-05-15 | Published at: 2026-06-01
Abstract: This retrospective comparative study evaluated postoperative intraocular pressure (IOP) control following trabeculectomy with mitomycin C (TRAB+MMC) versus deep sclerectomy with mitomycin C (DS+MMC) in patients with advanced uncontrolled primary open-angle glaucoma at Tripoli Eye Hospital during 2021–2022. Thirty eyes were included and equally divided between the two surgical groups, with postoperative follow-up extending to six months. Surgical success was defined as achieving and maintaining a target IOP of 10–15 mmHg without additional antiglaucoma medication, needling, or bleb revision. Both procedures produced a marked early reduction in IOP, particularly on the first postoperative day and during the first month, with most eyes reaching the target pressure range. However, trabeculectomy demonstrated superior long-term pressure control, with a higher proportion of eyes maintaining target IOP at three and six months compared with deep sclerectomy. By the sixth month, the DS group showed a higher rate of IOP elevation above 20 mmHg, requiring the addition of one or two antiglaucoma medications. Postoperative complications were observed only in the TRAB+MMC group, including one case of hypotony with shallow anterior chamber and two cases of elevated IOP requiring bleb revision with MMC; all were successfully managed. No postoperative complications were reported in the DS+MMC group. The findings suggest that TRAB+MMC provides more effective medium-term IOP control in advanced open-angle glaucoma, while DS+MMC offers a safer postoperative profile but may have lower durability in maintaining target IOP without medication. Larger prospective studies with longer follow-up are recommended to confirm these findings and better define the role of each procedure in glaucoma surgical management.
Keywords: Glaucoma; intraocular pressure; trabeculectomy; deep sclerectomy; mitomycin C; open-angle glaucoma.
المستخلص: هدفت هذه الدراسة المقارنة الاسترجاعية إلى تقييم التحكم في ضغط العين بعد الجراحة لدى المرضى الذين خضعوا لعملية استئصال التربيق باستخدام الميتومايسين C مقارنةً بعملية استئصال الصلبة العميق باستخدام الميتومايسين C، وذلك لدى حالات الزَّرَق مفتوح الزاوية الأولي المتقدم وغير المسيطر عليه في مستشفى طرابلس للعيون خلال الفترة 2021–2022. شملت الدراسة ثلاثين عينًا قُسِّمت بالتساوي بين المجموعتين الجراحيتين، مع متابعة ما بعد الجراحة لمدة ستة أشهر. وقد عُرِّف النجاح الجراحي بأنه الوصول إلى ضغط عين مستهدف يتراوح بين 10 و15 ملم زئبق والمحافظة عليه دون الحاجة إلى أدوية إضافية مضادة للزرق، أو تدخل بالإبرة، أو إصلاح للفقاعة الترشيحية. أظهرت كلتا العمليتين انخفاضًا واضحًا ومبكرًا في ضغط العين، لا سيما في اليوم الأول والشهر الأول بعد الجراحة، حيث وصلت معظم العيون إلى نطاق الضغط المستهدف. ومع ذلك، أظهرت عملية استئصال التربيق تفوقًا في التحكم بضغط العين على المدى المتوسط، إذ حافظت نسبة أعلى من العيون على الضغط المستهدف عند الشهرين الثالث والسادس مقارنةً بمجموعة استئصال الصلبة العميق. وبحلول الشهر السادس، سجّلت مجموعة استئصال الصلبة العميق نسبة أعلى من ارتفاع ضغط العين إلى أكثر من 20 ملم زئبق، مما استدعى إضافة دواء أو دواءين من الأدوية المضادة للزرق. أما المضاعفات بعد الجراحة فقد ظهرت فقط في مجموعة استئصال التربيق باستخدام الميتومايسين C، وشملت حالة واحدة من انخفاض ضغط العين مع ضحالة الحجرة الأمامية، وحالتين من ارتفاع ضغط العين احتاجتا إلى إصلاح الفقاعة الترشيحية باستخدام الميتومايسين C، وقد تمت السيطرة على جميع الحالات بنجاح. ولم تُسجَّل أي مضاعفات بعد الجراحة في مجموعة استئصال الصلبة العميق. تشير نتائج الدراسة إلى أن استئصال التربيق باستخدام الميتومايسين C يحقق فعالية أكبر في التحكم بضغط العين على المدى المتوسط لدى حالات الزرق مفتوح الزاوية المتقدم، في حين يتميز استئصال الصلبة العميق باستخدام الميتومايسين C بملف أمان أفضل بعد الجراحة، لكنه قد يكون أقل قدرة على المحافظة المستمرة على ضغط العين المستهدف دون علاج دوائي. وتوصي الدراسة بإجراء دراسات مستقبلية على عينات أكبر وبفترات متابعة أطول لتأكيد هذه النتائج وتحديد الدور الأمثل لكل إجراء جراحي في علاج الزرق.
الكلمات المفتاحية: الزرق؛ ضغط العين؛ استئصال التربيق؛ استئصال الصلبة العميق؛ الميتومايسين C؛ الزرق مفتوح الزاوية.
INTRODUCTION and STATEMENT OF PROBLEM;
Glaucoma is the silent thief of vision for decades as its considered the most common cause of irreversible blindness worldwide and even in Libya according to a study had held in 4 different cities 2013, represents the most common causes of loss of vision after cataract was due to glaucoma 24% .Since the only modifiable factor in this devastating blinding disease was found the Intra ocular pressure (IOP),So the key is controlling it to stop the disease progress ,however, its control must be either medically ,laser treatment or surgically .
in this comparative study all cases were in the advanced stage of glaucoma on triple or more medication with lake of IOP control and the disease was progressing by the time ,as a result surgical intervention was the only option to be applied .
in TRIPOLI EYE HOSPITAL the only surgical methods were available (conventional trabeculectomy (TRAB)or TRAB augmented with MMC and Ahmed Valves . Recently, nonpenetrating glaucoma filtration surgery(NPGFS) has been introduced at Tripoli eye hospital Since 2021 ,like Deep sclerectomy (DS) with MMC (mitomycin; anti metabolites) its Alkylating agent that inhibit DNA replication to help counter fibroblasts involved in scarring process at the filtrating surgical site, thereby improving surgical success according to UK NICE guidelines NG81 recommendations. Although, TRAB+ MMC is considered the gold standard surgical method in this research we would like to compare it to NPGS to prove the efficacy and safety to our patents in the hospital in order to achieve the best target post operative IOP results.
This study explore the 6month period target IOP control achieved post surgically comparing TRAB +MMC to DS+MMC at a single tertiary eye hospital in Tripoli Libya.
Methods:
A comparative retrospective study was held in TRIPOLI EYE HOSPITAL in 2021_2022 analysing30 eyes were operated in the hospital divided between TRABECULECTOMY ( TRAB) and DEEP SCLERECTOMY (DS) with Mitomycin respectively ,as registered and reviewed via hospital records, follow up period was six months. The participants were randomly selected in the glaucoma clinic all of them were advanced primary open angle Glaucoma(POAG) with lake of IOP control despite using triple treatment or more .All preoperative assessments were performed ,start from visual acuity ,slit lamp examination, Gonioscopy, fundoscopy ,ends with diagnostic investigation like (pachmetry,visual field 24′-2 for V/A <6/60 ,10′-2 for advanced cases, NFL OCT ).All patients who were 2ry open or closed angle Glaucoma, past medical history ,or previous glaucoma filtration surgery were excluded.
The surgeries were performed by different surgeons following the same surgical technique and guidelines of both previously mentioned surgeries .Surgical success was defined as IOP ≤10-15mmHg since day one and maintained to the 3rd till 6th months after surgery without medication needling or bleb revision the outcome addressed both IOP control and changes as well as managing post op complications .
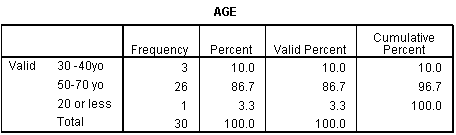
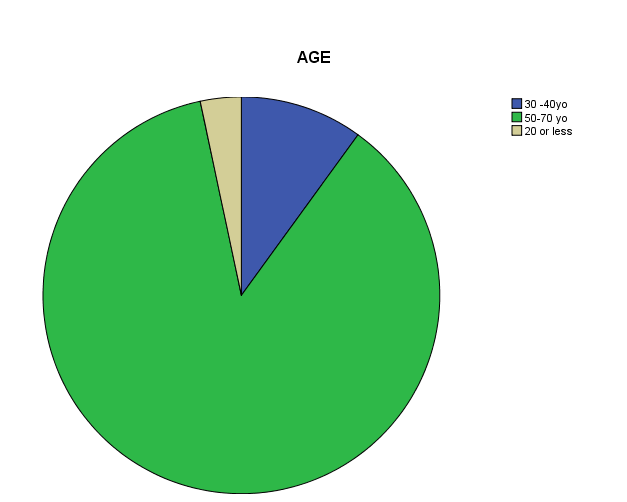
Statistical analysis was performed by SPSS 16 ,DATA introduced (ID ,AGE mean was ≤50-70yo,BCVA 6/24-6/60 93.2 % ,6.7 %<6/60 Snellen chart, Gender 76.7% were female while 23.3% male ,preoperative IOP 80%> than 20mmHg,gonioscopy (OAG) ,type of surgeries (TRAB,DS+MMC) and post operative IOP 1st day ,month,3rd month,6th month follow up ,Post op complications 90% no complications .Pearson chi-square test were used to assess differences between 2 surgical groups for baseline variables .A P value was <0.05 was considered statistically significant. All conducted with adherent to the tents of the Declaration of Helsinki.
Surgical technique of T trabeculectomy with mitomycin C
Under complete Aseptic technique. A 8-0 Vicryl corneal traction suture was performed all the surgical area was exposed conjunctival peritomy with tenon fornix based approach flab created, then hemostasis achieved by cauterization ,4×4 scleral flab 2/3 thickness, next MMC 0.2mg/ml, small sponge socked in inserted beneath the flab for 2 minutes ,next frequent copious irrigation .A paracentesis is performed and the anterior chamber was entered. Ostium fashioning using Kelly punch, followed by peripheral iridectomy ,10-0 nylon suture were used to close the scleral flab at apices next checking the flab leak by saline through paracentesis if it needs more stitches approximation of the conjunctival with Tenon using 8-0 vicryl last hydration of paracentesis, sub conjunctival steroid with antibiotic injected.
Surgical technique of Deep sclerectomy +MMC
Corneal traction suture 8-0 Vicryl was placed superiorly followed by fornix base conjunctival flab creation, cautery to achieve hemostasis ,then 4×4mm scleral flab was done half thickness limbus-based superficial flab and advanced 1mm to the clear cornea ,0.2 mg/ml MMC soaked sponges inserted for 2minutes applied posteriorly under conjunctiva and scleral flab then copious irrigation by BSS .Next , deep scleral flab 3×3mm had been created to the level of Schlemm’s canal ,de roofing with with removal of fibers at Trabeculodesment’s window, percolation of aqueous will be obvious after that tight superficial scleral flab sutured with10-0 nylon then conjunctival sutured with 8-0 vicryl tightly .Sub conj steroid with antibiotic injected.
Results:
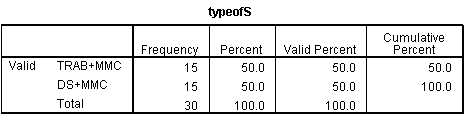
A total 30 eyes analyzed, which included 15deep sclerectomy group and 15 TRAB+MMC group.
All variables in both groups are listed in tables and charts below.
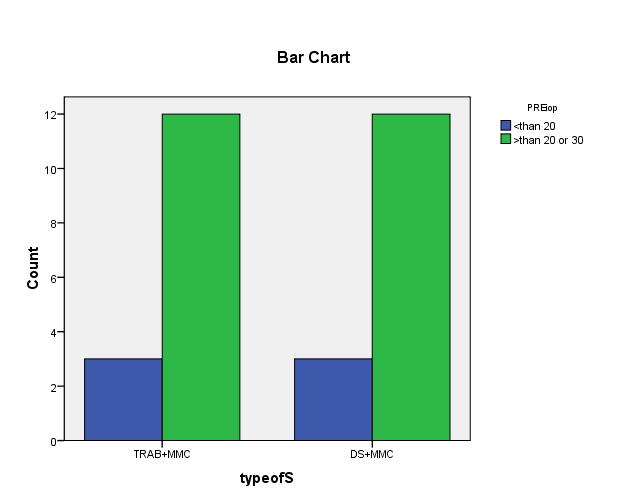
Preop- IOP
TRAB+MMC and DS+MMC groups preoperative IOP which 80% >20mmHg that shows almost 73% IOP reduction post operative, in which was striking reduction almost similarly in both previously mentioned procedures in the early days post op.
TRAB+mmc VS DS +mmc post operative IOP from 1st day up to the 6th month table and charts respectively :
|
Post operative IOP |
TRAB+MMC |
DS+MMC |
P value |
|
1st day 8-10mmHg 10-15mmHg >20mmHg |
55.6% 50% 0% |
44.45 50% 0% |
0.52 |
|
1st MON 8-10mmHg 10-15mmHg >20mmHg |
50% 60% 0% |
50% 40% 13.3% |
0.09 |
|
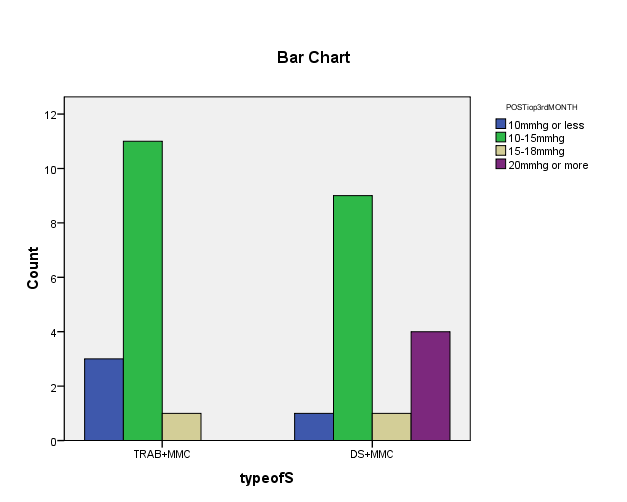
3rd MON 8-10mmhg 10-15mmHg >20mmHg |
66.7% 33% 0% |
33.3% 46.7% 20% |
0.04 |
|
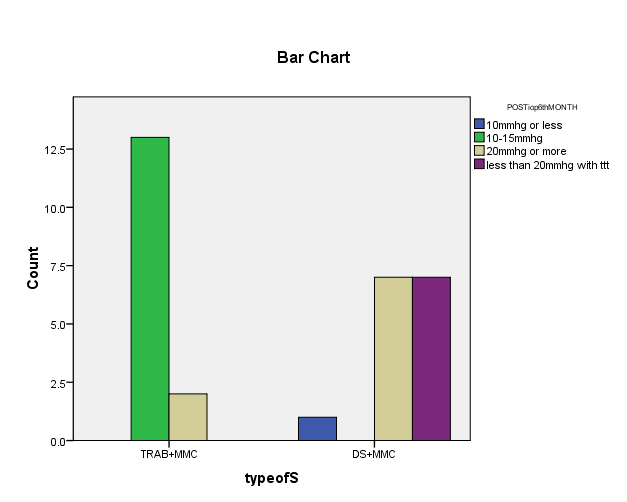
6th MON 8-10mmHg 10-15mmHg >20mmHg |
80% 20% 0% |
20% 40% 66% |
0.01 |
TRAB+MMC vs DS+MMC post operative IOP target control since day one till the 6th month follow up represents TRAB group significantly reach the target IOP control between 10-15 mmHg without medication compared to deep sclerectomy group. The p value is significant since 1st month which was <0.5.
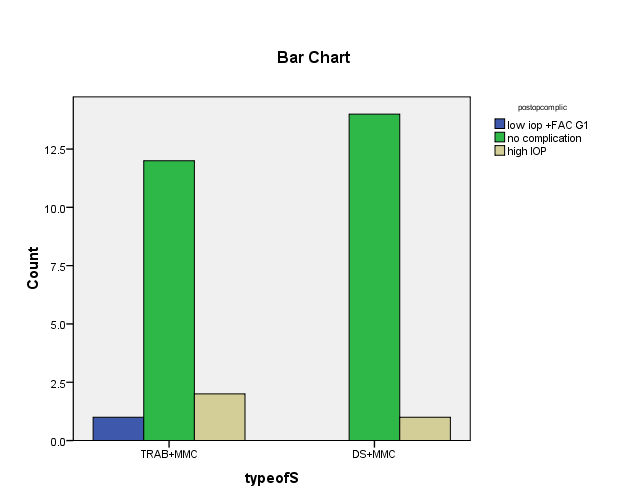
Post operative complications:
Generally, no complications had observed in deep sclerectomy group post operative as it’s common complications appears intraoperative which conclude, either trabeculodescemet’s meshwork (TDM) perforation, or difficulties in identification of Schlemm’s canal that fortunately both hadn’t occurred. Nevertheless, DS group fail to maintain target IOP additionally to the high IOP by the end of 1st month that controlled by adding one or maximum 2 drops which show statistic drops reduction. However, in TRAB group luckily 80% had no complications only 3 cases; one case with FAC G1 in which managed with Atropine 1% 1×4 and steroid drops after one week the A/C maintained the other 2 patients presented with High spikes of IOP ≥25mmHg that managed with bleb revision and poster post op MMC injection after 2 weeks then the IOP decline to normal had been noticed.
Key Words; post-op, TRAB VS DS complications, epidemiological studies, comparison.
Conclusion:
To conclude that TRAB+MMC achieved the best intraocular pressure success control on the long term duration follow up in comparison to deep sclerectomy+ MMC ,which achieve the target IOP only in the early period then spikes of high IOP > than 20 mmHg registered after the 1st month that controlled by anti-glaucoma treatment to be ≤21mmhg,however, post operative complication noticed in TRAB group which managed , to control the IOP one case with ATROPIN drops 2 cases with Bleb revision augmented with MMC ,compared to DS no any complication had found like shallow anterior chamber , that makes the deep sclerectomy has high safety profile.
Recommendation and weakness:
The sample analyzed it’ would be better to be larger, as well as the follow up period to be longer for many years so the result will be statically more sensible and accurate .However, in most previously comparative studies there were limitless either short duration or small sample .Moreover ,some of the founded long retrospective studies represents the efficacy of TRAB+MMC IOP reduction compared to DS+MMC that have more safety profile with success on the number of anti-glaucoma treatment ,which was considered in some studies surgical success. Some of confounding factors wasn’t taken in to considerations such as race which might had an effect on the post operative pressure control and the failure rate.
References:
- American Academy of Ophthalmology. Understanding glaucoma: symptoms, causes, diagnosis, treatment. American Academy of Ophthalmology; 2026. Available from: AAO Eye Health.
- Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P71–P150.
- Dwivedi R, Somerville T, Cheeseman R, Rogers C, Batterbury M, Choudhary A. Deep sclerectomy and trabeculectomy augmented with Mitomycin C: 2-year post-operative outcomes. Graefe’s Archive for Clinical and Experimental Ophthalmology. 2021;259:1965–1974. doi:10.1007/s00417-021-05144-w.
- El Sayyad F, Helal M, El-Kholify H, Khalil M, El-Maghraby A. Nonpenetrating deep sclerectomy versus trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology. 2000;107:1671–1674.
- Chiselita D. Nonpenetrating deep sclerectomy versus trabeculectomy in primary open-angle glaucoma surgery. Eye. 2001;15:197–201.
- Varga Z, Shaarawy T. Deep sclerectomy: safety and efficacy. Middle East African Journal of Ophthalmology. 2009;16(3):123–126. doi:10.4103/0974-9233.56223.
- Mendrinos E, Mermoud A, Shaarawy T. Nonpenetrating glaucoma surgery. Survey of Ophthalmology. 2008;53(6):592–630.
- Mendrinos E, Shaarawy T. The current situation in non-penetrating glaucoma surgery. European Ophthalmic Review. 2009;2(1):35–38. doi:10.17925/EOR.2009.02.01.35.
- Anand N, Atherley C. Deep sclerectomy augmented with mitomycin C. Eye. 2005;19:442–450. doi:10.1038/sj.eye.6701403.
- Gandolfi SA. Deep sclerectomy vs trabeculectomy in open-angle glaucoma: 7-year follow-up. Investigative Ophthalmology & Visual Science. 2005;46:1217.
- Mermoud A, Schnyder CC, Sickenberg M, Chiou AGY, Hédiguer SEA, Faggioni R. Comparison of deep sclerectomy with collagen implant and trabeculectomy in open-angle glaucoma. Journal of Cataract and Refractive Surgery. 1999;25:323–331. doi:10.1016/S0886-3350(99)80079-0.
- Ambresin A, Shaarawy T, Mermoud A. Deep sclerectomy with collagen implant in one eye compared with trabeculectomy in the other eye of the same patient. Journal of Glaucoma. 2002;11:214–220.
- Cillino S, Di Pace F, Casuccio A, Lodato G. Deep sclerectomy versus punch trabeculectomy with and without phacoemulsification: a randomized clinical trial. Journal of Glaucoma. 2004;13:500–506.
- Shaarawy T, Mansouri K, Schnyder C, Ravinet E, Achache F, Mermoud A. Long-term results of deep sclerectomy with collagen implant. Journal of Cataract and Refractive Surgery. 2004;30(6):1225–1231.
- Shaarawy T, Karlen M, Schnyder C, Achache F, Sanchez E, Mermoud A. Five-year results of deep sclerectomy with collagen implant. Journal of Cataract and Refractive Surgery. 2001;27(11):1770–1778.
- Anand N, Atherley C. Deep sclerectomy augmented with mitomycin C. Eye. 2005;19:442–450. doi:10.1038/sj.eye.6701403.